
Forum Members!


















Who We Are
Our Current Initiatives
The HCPLAN launched four new initiatives, spearheaded by leaders in the private, public, and non-profit sectors, committed to driving positive change.

10 Years of Collaboration,
Progress, and Advancing
Value-Based Care
Take a look back at our journey in our anniversary milestone video.
Explore HCPLAN Resources

Connect with the HCPLAN
Stay in the loop by following the HCPLAN on LinkedIn for news, insights, and events.
![]()
![]()
A decade ago, leaders across the health care industry came together around a shared goal: transforming how the nation pays for care.
What began as a collaborative effort to align stakeholders across the industry… Read More
![]()
![]()
Looking for resources, tools, and insights related to #ValueBasedCare?
The HCPLAN resource library brings together publications, frameworks, tools, and materials to support learning, collaboration, and… Read More
![]()
![]()
Collaboration across the health care system is essential to advancing #ValueBasedCare.
The HCPLAN’sThe HCPLAN’s newest resource tackles a critical challenge: How do we systematically move preventive… Read More
What is value-based payment?
Value-based payment refers to payment models that reward providers for delivering high-quality, efficient care rather than paying primarily for the volume of services delivered. These models often link payment to patient outcomes, care coordination, and cost management, helping improve quality while controlling health care spending.
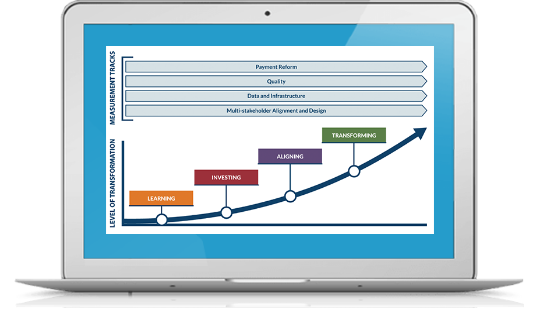
What is accountable care?
Accountable care is centered on the patient and aligns their care team to support shared decision-making and to realize the highest achievable health outcomes for all through comprehensive, high-quality, affordable, longitudinal care. The HCPLAN developed the Accountable Care Curve as a resource to help stakeholders drive the adoption of accountable care through a four step framework: learning, investing, aligning, and transforming.
How can I get involved with the HCPLAN?
Interested individuals and organizations can sign up for the HCPLAN email listserv and follow us on LinkedIn. If you are working on any of the current initiatives areas, the HCPLAN would love to hear from you. You can get in touch here.











 Emily DuHamel Brower, M.B.A., is senior vice president of clinical integration and physician services for Trinity Health. Emphasizing clinical integration and payment model transformation, Ms. Brower provides strategic direction related to the evolving accountable healthcare environment with strong results. Her team is currently accountable for $10.4B of medical expense for 1.6M lives in Medicare Accountable Care Organizations (ACOs), Medicare Advantage, and Medicaid and Commercial Alternative Payment Models.
Emily DuHamel Brower, M.B.A., is senior vice president of clinical integration and physician services for Trinity Health. Emphasizing clinical integration and payment model transformation, Ms. Brower provides strategic direction related to the evolving accountable healthcare environment with strong results. Her team is currently accountable for $10.4B of medical expense for 1.6M lives in Medicare Accountable Care Organizations (ACOs), Medicare Advantage, and Medicaid and Commercial Alternative Payment Models. Victor is the Chief Medical Officer for TennCare, Tennessee’s Medicaid Agency. At TennCare, Victor leads the medical office to ensure quality and effective delivery of medical, pharmacy, and dental services to its members. He also leads TennCare’s opioid epidemic strategy, social determinants of health, and practice transformation initiatives across the agency. Prior to joining TennCare, Victor worked at Evolent Health supporting value-based population health care delivery. In 2013, Victor served as a White House Fellow to the Secretary of Health and Human Services. Victor completed his Internal Medicine Residency at Emory University still practices clinically as an internist in the Veteran’s Affairs Health System.
Victor is the Chief Medical Officer for TennCare, Tennessee’s Medicaid Agency. At TennCare, Victor leads the medical office to ensure quality and effective delivery of medical, pharmacy, and dental services to its members. He also leads TennCare’s opioid epidemic strategy, social determinants of health, and practice transformation initiatives across the agency. Prior to joining TennCare, Victor worked at Evolent Health supporting value-based population health care delivery. In 2013, Victor served as a White House Fellow to the Secretary of Health and Human Services. Victor completed his Internal Medicine Residency at Emory University still practices clinically as an internist in the Veteran’s Affairs Health System. Tamara Ward is the SVP of Insurance Business Operations at Oscar Health, where she leads the National Network Contracting Strategy and Market Expansion & Readiness. Prior to Oscar she served as VP of Managed Care & Network Operations at TriHealth in Southwest Ohio. With over 15 years of progressive health care experience, she has been instrumental driving collaborative payer provider strategies, improving insurance operations, and building high value networks through her various roles with UHC and other large provider health systems. Her breadth and depth of experience and interest-based approach has allowed her to have success solving some of the most complex issues our industry faces today. Tam is passionate about driving change for marginalized communities, developing Oscar’s Culturally Competent Care Program- reducing healthcare disparities and improving access for the underserved population. Tamara holds a B.A. from the University of Cincinnati’s and M.B.A from Miami University.
Tamara Ward is the SVP of Insurance Business Operations at Oscar Health, where she leads the National Network Contracting Strategy and Market Expansion & Readiness. Prior to Oscar she served as VP of Managed Care & Network Operations at TriHealth in Southwest Ohio. With over 15 years of progressive health care experience, she has been instrumental driving collaborative payer provider strategies, improving insurance operations, and building high value networks through her various roles with UHC and other large provider health systems. Her breadth and depth of experience and interest-based approach has allowed her to have success solving some of the most complex issues our industry faces today. Tam is passionate about driving change for marginalized communities, developing Oscar’s Culturally Competent Care Program- reducing healthcare disparities and improving access for the underserved population. Tamara holds a B.A. from the University of Cincinnati’s and M.B.A from Miami University.


 Dr. Peter Walsh joined the Colorado Department of Health Care Policy and Financing as the Chief Medical Officer on December 1, 2020. Prior to joining HCPF, Dr. Walsh served as a Hospital Field Representative/Surveyor at the Joint Commission, headquartered in Oakbrook Terrace, Illinois.
Dr. Peter Walsh joined the Colorado Department of Health Care Policy and Financing as the Chief Medical Officer on December 1, 2020. Prior to joining HCPF, Dr. Walsh served as a Hospital Field Representative/Surveyor at the Joint Commission, headquartered in Oakbrook Terrace, Illinois.





