
Accelerating and Aligning
Clinical Episode Payment Models
Chapter 5: Coronary Artery Disease
Report: Released August 1, 2016
Chapter Description
According to the National Center for Chronic Disease Prevention and Health Promotion’s Division for Heart Disease and Stroke Prevention, coronary artery disease (CAD) is the most common type of heart disease in America. In the United States in 2010, about 20% of the 65-year-old and over population were living with CAD. This condition is also present in about 7% of the population who are between the ages of 45 and 64. The two procedures most commonly used to treat CAD patients—PCI and CABG—account for more than one million procedures done annually in the United States.
Episode payment for CAD establishes a budget that incentivizes the providers managing the patient to more appropriately balance the needs of the patient and the number and type of services provided. Placing accountability for the entire condition with a designated provider also encourages the active management of the patient in order to prevent acute events that lead to worsening health, further procedures, and an increased risk of overall poor outcomes. The goal of person-centered episode payment is to make the patient the focus of care management, ensuring that any efficiencies achieved through improved care coordination and management first and foremost benefit the patient.
Authors
Publication Info
Publication date: August 1, 2016
Pages 66-92
Suggested Citation: Health Care Payment Learning & Action Network. Accelerating and Aligning Clinical Episode Payment Models.
August 1, 2016.
Accountable Entity
The accountable entity should be chosen based on its ability to engineer change in the way care is delivered to the patient and its ability to accept risk for an episode of care. The cardiologist or primary care provider may be best positioned to play this role and should be accountable for overall outcomes, including sharing accountability for the procedure with the intensivist or cardiothoracic surgeon.
Acute Care Episode (ACE) Demonstration
This bundled payment approach includes 28 cardiac and nine orthopedic inpatient surgical services and procedures.
Appropriate Use Criteria Guidelines
The Appropriate Use Criteria Guidelines were developed by a consortium that includes the American College of Cardiology Foundation, the Society for Cardiovascular Angiography and Interventions, the Society of Thoracic Surgeons, the American Association for Thoracic Surgery, the American Heart Association, the American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography.
CABG
Coronary artery bypass graft
CAD
Coronary artery disease
Clinical Episode Payment
A clinical episode payment is a bundled payment for a set of services that occur over time and across settings. This payment model can be focused on a: setting (such as a hospital or a hospital stay); procedure (such as elective surgery); or condition (such as diabetes).
Clinical Episode Payment Work Group
The LAN Guiding Committee convened the Clinical Episode Payment (CEP) Work Group to create a set of recommendations that can facilitate the adoption of clinical episode-based payment models.
Clinical Episode Payment Models
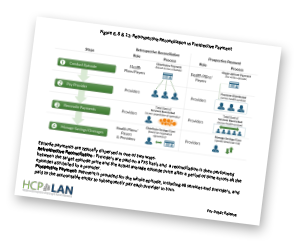
Clinical episode payment models are different from traditional fee-for-service (FFS) health care payment models, in which providers are paid separately for each service they deliver. Instead, clinical episode payment models take into consideration the quality, costs, and outcomes for a patient-centered course of care over a set period of time and across multiple settings.
Condition and Procedure
The CAD episode described in this paper combines condition-level management with a “nested” bundle for the payment of a procedure, if one is deemed necessary and appropriate.
Condition: Patients diagnosed with CAD and in same health plan for full 12 months.
Procedure: Patients deemed to need a PCI or CABG based on appropriate use guidelines.
Core Set of Logic
This will assist the industry in developing the capacity for grouping claims into bundles by standardizing some of the logic and allowing each payer to customize some of the more specific rules.
Design Elements
The design elements address questions stakeholders must consider when designing an episode payment model, including the definition, the duration of the episode, and what services are to be included.
Episode Price
The episode price should strike a balance between provider-specific and multi-provider/regional utilization history. The episode price should be set at a level that acknowledges achievable efficiencies already gained by previous programs; and reflects a level that potential provider participants see as feasible to attain.
Episode Timing
The condition episode commences at the beginning of the first benefit year post-CAD diagnosis, and lasts for 12 months. The procedure episode begins 30-days pre-procedure and lasts 30-90 days post-discharge.
Episodes of Care
The CAD episode proposed by the CEP Work Group combines condition-level management with a nested procedure bundle. This is an important distinction from the majority of existing CAD-related episode payment models, which focus solely on PCI or CABG.
Fee-for-Service (FFS)
Traditional FFS creates incentives for providing a high quantity of services and treatments, potentially rewarding the use of expensive treatments and tests regardless of value to the patient, as well as avoidable invasive procedures and hospitalizations.
Operational Considerations
Operational considerations relate to implementing an episode payment model, including the roles and perspectives of stakeholders, data infrastructure issues, and the regulatory environment in which APMs must operate.
PCI
Percutaneous coronary intervention
Quality Metrics
These include outcome metrics, patient-reported outcome and functional status measures, and some process measures related to the procedures.
Clinical episode payment models are different from traditional fee-for-service (FFS) health care payment models in which providers are paid separately for each service they deliver. Instead, clinical episode payment models take into consideration the quality, costs, and outcomes for a patient-centered course of care over a set period of time and across multiple settings. This course of care is known as the clinical episode. Research suggests that when payments for health care are based on the care delivered in a clinical episode, the result is increased coordination of care, enhanced quality of care, and less fragmentation in the medical system. This leads to better experience and health for patients and lower costs for payers and providers.




Figure 9:
Nested CAD
Episode
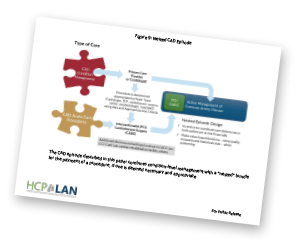
Figure 10:
CAD Episode
Timeline

Figure 11:
Retrospective Reconciliation vs. Prospective Payment
How did the LAN determine which quality measures to include in the CAD recommendations?
The CAD condition and procedure-related quality measures that are listed in the Chapter 5 Quality Metrics recommendations are offered as suggestions for potential use for accountability and/or payment. This is not an all-inclusive list of measures. The LAN recommends that this list be used as a discussion point for stakeholders to determine which quality metrics would best measure improvement in the services being delivered in this episode. It is important to consider the concerns and gain consensus across all stakeholder groups when determining which quality metrics are critical to the success of an episode model.
How do the LAN recommendations on Coronary Artery Disease (CAD) episode payment address the issue of assessing whether a CAD procedure is appropriate and necessary?
The LAN recommendations on CAD episode payment reflect the concern that some CAD PCI and/or CABG procedures are conducted when not clinically necessary. Therefore, the recommendations discuss the need for determining if a PCI or CABG procedure is necessary via consultation both within a “Heart Team” (composed of the referring physicians, cardiothoracic surgeons, cardiologists, cardiac anesthesiologist and hospitalists, and any other health care providers who may be integral to the patient’s care) and between the Heart Team and the patient and patient’s family. The recommendations also discuss the importance of the Heart Team applying Appropriate Use Criteria and other relevant clinical practice guidelines. The use of an innovative model such as the “Heart Team” will likely require that the associated costs be included when calculating the episode price.
Why does the CAD episode begin at a period of time post-diagnosis instead of at the point of diagnosis?
The Episode Timing recommendation suggests two different options for setting the episode period. Both options are intended to simplify the operationalization of the episode, and the entity implementing the bundle must decide which method would be appropriate for their patient population. The first option is to begin the bundle at the start of the next benefit year, which for a health plan, would help align the timing of the episode with the timing of the benefit year. Resource use should be monitored in the time between diagnosis and enrollment in the bundle to discourage unintended consequences. One such unintended consequence may be an increase in the number of procedures or services performed between diagnosis and enrollment in order to receive the FFS pricing outside of the bundle. The second option is to begin the episode on the first day of the next month (or first day of the next quarter). While this option would require a rolling enrollment period which may be more difficult operationally for certain implementers, it may help address the issue of over- or underutilization of services before enrollment in the episode of care. It should be noted that this explanation refers only to the CAD condition. If a PCI or CABG procedure is necessary, the White Paper defines specific recommendations of when the timing of those episodes should start in the bundle based on whether the procedure is elective or emergent. These recommendations were suggested after a careful review of PCI and CABG bundles that are currently in use.
How do the LAN recommendations address the variation and severity of CAD across the patient population?
The LAN acknowledges that there is wide variation in the severity of CAD across the patient population, which could affect episode pricing and the types of services that an accountable entity would want to consider including in the bundle. To address this, the recommendation supports the use of patient cohorts to group patients. These cohorts may be organized by patients with stable CAD vs patients with unstable CAD, or by the type (i.e. medical vs. surgical) or number of treatments a patient is receiving. The Patient Population design element recommendation includes further details about establishing patient cohorts.
Webinars
March 2016 Webinar: LAN Update: Episode Bundles – Why It Matters and What Purchasers Can Do Now (archive)
April 2016 Webinar: LAN Summit Session for States: When APMs Intersect– The Challenges and Opportunities of Implementing Episode Payment in a Population-Based Payment Environment (archive)
April 2016 Webinar: LAN Summit Session: Improving the Delivery of Cardiac Care Via Episode Payment Opportunities and Challenges (archive)
June 2016 Webinar: LAN Listening Session: Opportunities & Challenges in Cardiac Care Episode Payments (archive)
Blogs
Lowering Costs and Improving Care Through Episode/Bundled Payments
by Lewis Sandy, MD, MBA
Archival Materials
Draft Paper: Accelerating and Aligning Clinical Episode Payment Models: Coronary Artery Disease
Summary of Public Comments: Summary of Public Comments
















 Emily DuHamel Brower, M.B.A., is senior vice president of clinical integration and physician services for Trinity Health. Emphasizing clinical integration and payment model transformation, Ms. Brower provides strategic direction related to the evolving accountable healthcare environment with strong results. Her team is currently accountable for $10.4B of medical expense for 1.6M lives in Medicare Accountable Care Organizations (ACOs), Medicare Advantage, and Medicaid and Commercial Alternative Payment Models.
Emily DuHamel Brower, M.B.A., is senior vice president of clinical integration and physician services for Trinity Health. Emphasizing clinical integration and payment model transformation, Ms. Brower provides strategic direction related to the evolving accountable healthcare environment with strong results. Her team is currently accountable for $10.4B of medical expense for 1.6M lives in Medicare Accountable Care Organizations (ACOs), Medicare Advantage, and Medicaid and Commercial Alternative Payment Models. Mr. James Sinkoff is the Deputy Executive Officer and Chief Financial Officer for Sun River Health (formerly known as Hudson River HealthCare), and the Chief Executive Officer of Solutions 4 Community Health (S4CH); an MSO serving FQHCs and private physician practices.
Mr. James Sinkoff is the Deputy Executive Officer and Chief Financial Officer for Sun River Health (formerly known as Hudson River HealthCare), and the Chief Executive Officer of Solutions 4 Community Health (S4CH); an MSO serving FQHCs and private physician practices. Victor is the Chief Medical Officer for TennCare, Tennessee’s Medicaid Agency. At TennCare, Victor leads the medical office to ensure quality and effective delivery of medical, pharmacy, and dental services to its members. He also leads TennCare’s opioid epidemic strategy, social determinants of health, and practice transformation initiatives across the agency. Prior to joining TennCare, Victor worked at Evolent Health supporting value-based population health care delivery. In 2013, Victor served as a White House Fellow to the Secretary of Health and Human Services. Victor completed his Internal Medicine Residency at Emory University still practices clinically as an internist in the Veteran’s Affairs Health System.
Victor is the Chief Medical Officer for TennCare, Tennessee’s Medicaid Agency. At TennCare, Victor leads the medical office to ensure quality and effective delivery of medical, pharmacy, and dental services to its members. He also leads TennCare’s opioid epidemic strategy, social determinants of health, and practice transformation initiatives across the agency. Prior to joining TennCare, Victor worked at Evolent Health supporting value-based population health care delivery. In 2013, Victor served as a White House Fellow to the Secretary of Health and Human Services. Victor completed his Internal Medicine Residency at Emory University still practices clinically as an internist in the Veteran’s Affairs Health System. Dr. Brandon G. Wilson, DrPH, MHA (he, him, his) joined Community Catalyst as the Director of the Center for Consumer Engagement in Health Innovation, where he leads the Center in bringing the community’s experience to the forefront of health systems transformation and health reform efforts, in order to deliver better care, better value and better health for every community, particularly vulnerable and historically underserved populations. The Center works directly with community advocates around the country to increase the skills and power they have to establish an effective voice at all levels of the health care system. The Center collaborates with innovative health plans, hospitals and providers to incorporate communities and their lived experience into the design of systems of care. The Center also works with state and federal policymakers to spur change that makes the health system more responsive to communities. And it provides consulting services to health plans, provider groups and other health care organizations to help them create meaningful structures for engagement with their communities.
Dr. Brandon G. Wilson, DrPH, MHA (he, him, his) joined Community Catalyst as the Director of the Center for Consumer Engagement in Health Innovation, where he leads the Center in bringing the community’s experience to the forefront of health systems transformation and health reform efforts, in order to deliver better care, better value and better health for every community, particularly vulnerable and historically underserved populations. The Center works directly with community advocates around the country to increase the skills and power they have to establish an effective voice at all levels of the health care system. The Center collaborates with innovative health plans, hospitals and providers to incorporate communities and their lived experience into the design of systems of care. The Center also works with state and federal policymakers to spur change that makes the health system more responsive to communities. And it provides consulting services to health plans, provider groups and other health care organizations to help them create meaningful structures for engagement with their communities. Tamara Ward is the SVP of Insurance Business Operations at Oscar Health, where she leads the National Network Contracting Strategy and Market Expansion & Readiness. Prior to Oscar she served as VP of Managed Care & Network Operations at TriHealth in Southwest Ohio. With over 15 years of progressive health care experience, she has been instrumental driving collaborative payer provider strategies, improving insurance operations, and building high value networks through her various roles with UHC and other large provider health systems. Her breadth and depth of experience and interest-based approach has allowed her to have success solving some of the most complex issues our industry faces today. Tam is passionate about driving change for marginalized communities, developing Oscar’s Culturally Competent Care Program- reducing healthcare disparities and improving access for the underserved population. Tamara holds a B.A. from the University of Cincinnati’s and M.B.A from Miami University.
Tamara Ward is the SVP of Insurance Business Operations at Oscar Health, where she leads the National Network Contracting Strategy and Market Expansion & Readiness. Prior to Oscar she served as VP of Managed Care & Network Operations at TriHealth in Southwest Ohio. With over 15 years of progressive health care experience, she has been instrumental driving collaborative payer provider strategies, improving insurance operations, and building high value networks through her various roles with UHC and other large provider health systems. Her breadth and depth of experience and interest-based approach has allowed her to have success solving some of the most complex issues our industry faces today. Tam is passionate about driving change for marginalized communities, developing Oscar’s Culturally Competent Care Program- reducing healthcare disparities and improving access for the underserved population. Tamara holds a B.A. from the University of Cincinnati’s and M.B.A from Miami University.


 Dr. Peter Walsh joined the Colorado Department of Health Care Policy and Financing as the Chief Medical Officer on December 1, 2020. Prior to joining HCPF, Dr. Walsh served as a Hospital Field Representative/Surveyor at the Joint Commission, headquartered in Oakbrook Terrace, Illinois.
Dr. Peter Walsh joined the Colorado Department of Health Care Policy and Financing as the Chief Medical Officer on December 1, 2020. Prior to joining HCPF, Dr. Walsh served as a Hospital Field Representative/Surveyor at the Joint Commission, headquartered in Oakbrook Terrace, Illinois.








