
Accelerating and Aligning
Population-Based Payment Models:
Data Sharing
Report: Released August 8, 2016
Description
Related Papers
The PBP Work Group authored four papers focusing on issues foundational to the success of PBP models. These include:
Authors
Publication Info
Publication date: August 8, 2016
43 pages
Suggested Citation: Health Care Payment Learning & Action Network. Accelerating and Aligning Population-Based Payment: Data Sharing.
August 8, 2016.
Table of Contents
About the CMS Alliance to Modernize Healthcare
Health Care Payment Learning & Action Network (LAN)
Purpose and Scope of the White Paper
Guiding Principles for Data Sharing
Data Sharing Organizational Profiles
Appendix C: LAN Related Content
Appendix D: Principles for Patient- and Family- Centered Payment
Alternative Payment Models (APMs)
Alternative payment models deviate from traditional fee-for-service (FFS) payment, insofar as they adjust FFS payments to account for performance on cost and quality metrics, or insofar as they use population-based payments that are linked to quality performance.
Data Sharing
Data sharing lies at the heart of two important and ambitious goals of PBP models and APMs: 1) It promotes the availability and use of real-time comprehensive, patient-level data and information to inform clinical care and decision making, enable true integration of care, and improve care delivery and outcomes; and 2) It improves the health care market, such that care is purchased on the basis of transparent and reliable assessments of cost and quality performance for populations.
Fee for Service (FFS)
The existing FFS system creates incentives for additional volume of services, while also undervaluing certain services. The current FFS system is not conducive to the delivery of person-centered care because it does not systematically reward high-quality, cost-effective care.
Full Continuum of Care
All aspects of care delivery, spanning preventive to end-of-life services in all settings.
Patient-Level Data
The entire range of diagnostic, clinical, utilization, experience of care, and patient-reported data that is attributed to a particular individual, irrespective of where the data were collected. Such data are stored in a cyber-secure, HIPAA-compliant environment to address security and privacy concerns and can be reported in both patient-identified and de-identified views.
Population-Based Payment (PBP)
Population-based payment models offer providers the incentives and flexibility to strategically invest delivery system resources, treat patients holistically, and coordinate care.
Population-Based Payment Model
A payment model in which a provider organization is given a population-based global budget or payment and accepts accountability for managing the total cost of care, quality, and outcomes for a defined patient population across the full continuum of care. PBP models discussed in this paper correspond to payment models in Categories 3 and 4 of the LAN’s APM Framework.
Population-Level Data
An aggregation of patient-level data, which is attributed to higher-level entities for reporting, such as plans, provider organizations, and patient populations in different geographic regions.
Total Cost of Care (TCOC)
A broad indicator of spending for a given population (i.e., payments from payer to provider organizations). In the context of PBP models, in which provider accountability spans the full continuum of care, TCOC includes all spending associated with caring for a defined population, including provider and facility fees, inpatient and ambulatory care, pharmacy, behavioral health, laboratory, imaging, and other ancillary services.
The LAN has written a suite of papers to help align payment reform efforts.
The papers include recommendations on the design of two payment reforms—population-based payments and clinical episode payments—from the two most comprehensive categories defined in that framework. These recommendations are the result of input from a wide variety of persons and organizations with either direct experience with implementing one or the other payment reform or deep experience in the health care field.



Briefing Deck – Population Based Payment Model
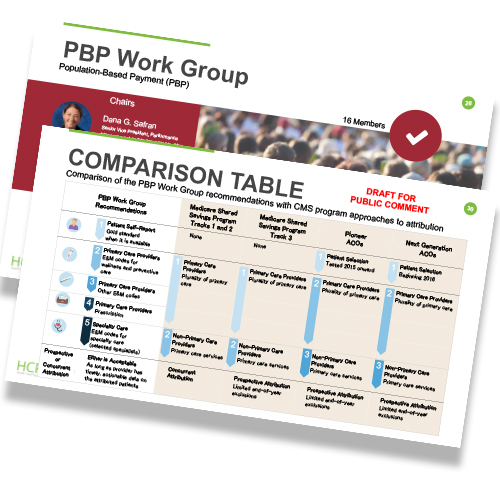
Figure 1: APM Framework (At-a-Glance)

Figure 2: Data Sharing is Foundational for Population-Based Payment

Figure 3: Data Sharing Use Cases at a Glance

Many of the Work Group’s recommendations for data sharing in Population-Based Payment (PBP) models could be applicable to data sharing in fee-for-service (FFS) models. Why does the White Paper not address how to improve data sharing in FFS models?
As noted in Principle 2, the Work Group believes that data sharing in PBP models will need to be fundamentally different than data sharing in FFS models. Although many aspects of the Work Group’s recommendations may in fact be important for FFS models, our charge was limited to recommendations on data sharing in PBP models.
What purpose does data sharing serve in a PBP model?
Data is absolutely essential for PBP models. In the first place, data sharing is necessary to operationalize essential elements of PBP models. Without data it is not possible to attribute patients to providers, assess performance on cost and quality, or other functions that need to be accomplished to run a PBP model. Moreover, data sharing beyond the bare necessities of operationalizing a PBP model will significantly improve stakeholders’ ability to reap these models’ full benefits. For example, access to cost and quality information substantially improves decision making for consumers and purchasers who are selecting providers and plans.
Why does the data sharing paper not address more of the "nuts and bolts” on how to enter into data-sharing agreements?
The Work Group does not believe that there is sufficient evidence to recommend a particular approach to entering into data sharing agreements or recruiting potential partners for data sharing. It is more appropriate for local decision-makers to take their particular circumstances into account when entering into data-sharing arrangements.
Is the Work Group proposing that data-sharing recommendations be the same or different for commercial and government payers?
The Work Group recognizes that statutory and regulatory constraints may limit the data sharing options available to public payers. However, the paper’s data-sharing recommendations are intended to apply to public and private payers alike.
Why did the Work Group focus on the “what” and the “who” and ignore the “how” of data sharing? Isn’t the “how” essential to help prospective advanced payment model (APM) adopters take the next step?
The Work Group acknowledges that the “how” of the complex challenge of data sharing needs to be addressed. We made the determination that it was essential to first to lay out the framework addressing the goals and outcomes. Because there are many different approaches to assessing and determining how to achieve these goals, the Health Care Payment Learning & Action Network (LAN) is committed to further work that will delve into “how” this may be achieved.
Is data for a 360-degree view of the patient, and especially a full clinical profile, necessary before providers can adopt a PBP model?
A comprehensive view is the ideal information status for maximizing value and east of operations within a PBP model. Having said that, providers and payers have already successfully adopted PBP work relationships in the absence of the ideal or comprehensive data view, so it is not absolutely essential for initiating the transition to PBP.
Is the LAN endorsing adoption of a national patient identifier?
The LAN recognizes the value offered by establishing a system for a national patient identifier, including safety through reducing errors related to treatment of patients with the same or similar names, by establishing linkages between different types of data (e.g., administrative and clinical data bases), and by eliminating one of the challenges standing in the way of data sharing between and among different provider and payer entities. Certain statutes are hindering progress in that area at present. Despite these constraints, the Work Group is aware of several health care organizations and states that have successfully engaged in data sharing using a local or regional identifier, and we believe that the adoption of PBP models can proceed, even in the absence of a national patient identifier.
How will payers, particularly competitors, be incentivized to cooperate in data-sharing agreements?
The Work Group believes that widespread adoption of PBP models will require a fundamental shift in business models, such that providers and payers compete on the basis of how well they make use of health data, as opposed to whether or not they are able to access it. When operating under such business models, competitors will have every incentive to cooperate by sharing data needed to make clinical decisions and manage populations health, and will instead compete on the basis of how well they are able to do so for their patient panels.
Does effective data sharing require robust sharing between multiple payers and multiple providers?
Yes, it will. This is especially the case for providers who participate in PBP models with multiple payers. In such cases, providers in PBP models will need to receive data from payers and providers that are outside of their network.
How do you propose addressing data sharing legal issues, particularly mental/behavioral health?
The Work Group recognizes that data sharing restrictions and adherence to Health Insurance Portability and Accountability Act (HIPAA) requirements can hinder complete data sharing among providers, thereby limiting full and transparent access by providers to the health needs and challenges of their patient population. This is an important policy issue spanning privacy, patient rights, data governance, and more that will need to be addressed on a forum beyond the LAN. This limitation however, should not interfere with movement toward adoption of Population-Based Payment models.
How can we ensure that the data being delivered is meaningful to the provider?
The Work Group recognizes that there are immense amounts of data available but it is often not particularly timely or usable for providers. There are many examples of dashboards and other data presentation formats that have been developed in some cases by third parties exclusively for the use of providers and are value-added to their clinical decision-making. Best practices can be derived from these prototypes and expect that future LAN work will highlight opportunities to learn from these successful efforts.
Why did the Work Group choose not address disparities in health care?
The focus of this paper was on payment reform, particularly the information exchange that takes place between providers and payers. Although data sharing may be used to reduce disparities, the Work Group did not explicitly consider this subject.
Why does the White Paper not address the high costs to providers, especially in small practices, of data sharing?
The White Paper focuses on the “who” and “what” needs to happen in conjunction with data sharing and less so on the “how.” Having said that, the Work Group has heard many concerns around prohibitive costs to smaller practitioners and will be taking that information forward to the LAN leadership to take into account in future data work.
Does the White Paper address the need to educate patients and their families about the value of data sharing?
The Work Group agrees that the long term success of PBP models requires patients and their families to understand the benefit that accrues to them when providers have access to comprehensive, longitudinal information about their conditions and treatments. Accordingly, Recommendation 3 calls for reaching a multi-stakeholder consensus on how to address patient concerns about privacy and the security of their personal health data. The Work Group envisions that educational initiatives for patients and family caregivers would naturally follow from this activity.
Webinars
November 2015 Webinar: LAN Learnings: Population-Based Payments (archive)
April 2016 Webinar: LAN Summit Session: When APMs Intersect: The Challenges and Opportunities of Implementing Episode Payment in a Population-Based Payment Environment (archive)
June 2016 Webinar: LAN Listening Session: Opportunities & Challenges in Data Sharing for Population-Based Payment Models (archive)
Blogs
Why Regional Data and Local Relationship Will Reform Health Care Payment Nationally
by Elizabeth Mitchell
Core Quality Measures Have Value for Alternative Payment Models
by Carmella Bocchino, RN, MBA; and Aparna Higgins
Population-Based Payment Models: Overcoming Barriers, Accelerating Adoption
by Dana Gelb Safran, ScD; Glenn Steele, Jr, MD, PhD; and Elizabeth Mitchell
Archival Materials
Draft Paper: Accelerating and Aligning Population-Based Payment Models: Data Sharing



 Emily DuHamel Brower, M.B.A., is senior vice president of clinical integration and physician services for Trinity Health. Emphasizing clinical integration and payment model transformation, Ms. Brower provides strategic direction related to the evolving accountable healthcare environment with strong results. Her team is currently accountable for $10.4B of medical expense for 1.6M lives in Medicare Accountable Care Organizations (ACOs), Medicare Advantage, and Medicaid and Commercial Alternative Payment Models.
Emily DuHamel Brower, M.B.A., is senior vice president of clinical integration and physician services for Trinity Health. Emphasizing clinical integration and payment model transformation, Ms. Brower provides strategic direction related to the evolving accountable healthcare environment with strong results. Her team is currently accountable for $10.4B of medical expense for 1.6M lives in Medicare Accountable Care Organizations (ACOs), Medicare Advantage, and Medicaid and Commercial Alternative Payment Models. Mr. James Sinkoff is the Deputy Executive Officer and Chief Financial Officer for Sun River Health (formerly known as Hudson River HealthCare), and the Chief Executive Officer of Solutions 4 Community Health (S4CH); an MSO serving FQHCs and private physician practices.
Mr. James Sinkoff is the Deputy Executive Officer and Chief Financial Officer for Sun River Health (formerly known as Hudson River HealthCare), and the Chief Executive Officer of Solutions 4 Community Health (S4CH); an MSO serving FQHCs and private physician practices. Victor is the Chief Medical Officer for TennCare, Tennessee’s Medicaid Agency. At TennCare, Victor leads the medical office to ensure quality and effective delivery of medical, pharmacy, and dental services to its members. He also leads TennCare’s opioid epidemic strategy, social determinants of health, and practice transformation initiatives across the agency. Prior to joining TennCare, Victor worked at Evolent Health supporting value-based population health care delivery. In 2013, Victor served as a White House Fellow to the Secretary of Health and Human Services. Victor completed his Internal Medicine Residency at Emory University still practices clinically as an internist in the Veteran’s Affairs Health System.
Victor is the Chief Medical Officer for TennCare, Tennessee’s Medicaid Agency. At TennCare, Victor leads the medical office to ensure quality and effective delivery of medical, pharmacy, and dental services to its members. He also leads TennCare’s opioid epidemic strategy, social determinants of health, and practice transformation initiatives across the agency. Prior to joining TennCare, Victor worked at Evolent Health supporting value-based population health care delivery. In 2013, Victor served as a White House Fellow to the Secretary of Health and Human Services. Victor completed his Internal Medicine Residency at Emory University still practices clinically as an internist in the Veteran’s Affairs Health System. Dr. Brandon G. Wilson, DrPH, MHA (he, him, his) joined Community Catalyst as the Director of the Center for Consumer Engagement in Health Innovation, where he leads the Center in bringing the community’s experience to the forefront of health systems transformation and health reform efforts, in order to deliver better care, better value and better health for every community, particularly vulnerable and historically underserved populations. The Center works directly with community advocates around the country to increase the skills and power they have to establish an effective voice at all levels of the health care system. The Center collaborates with innovative health plans, hospitals and providers to incorporate communities and their lived experience into the design of systems of care. The Center also works with state and federal policymakers to spur change that makes the health system more responsive to communities. And it provides consulting services to health plans, provider groups and other health care organizations to help them create meaningful structures for engagement with their communities.
Dr. Brandon G. Wilson, DrPH, MHA (he, him, his) joined Community Catalyst as the Director of the Center for Consumer Engagement in Health Innovation, where he leads the Center in bringing the community’s experience to the forefront of health systems transformation and health reform efforts, in order to deliver better care, better value and better health for every community, particularly vulnerable and historically underserved populations. The Center works directly with community advocates around the country to increase the skills and power they have to establish an effective voice at all levels of the health care system. The Center collaborates with innovative health plans, hospitals and providers to incorporate communities and their lived experience into the design of systems of care. The Center also works with state and federal policymakers to spur change that makes the health system more responsive to communities. And it provides consulting services to health plans, provider groups and other health care organizations to help them create meaningful structures for engagement with their communities. Tamara Ward is the SVP of Insurance Business Operations at Oscar Health, where she leads the National Network Contracting Strategy and Market Expansion & Readiness. Prior to Oscar she served as VP of Managed Care & Network Operations at TriHealth in Southwest Ohio. With over 15 years of progressive health care experience, she has been instrumental driving collaborative payer provider strategies, improving insurance operations, and building high value networks through her various roles with UHC and other large provider health systems. Her breadth and depth of experience and interest-based approach has allowed her to have success solving some of the most complex issues our industry faces today. Tam is passionate about driving change for marginalized communities, developing Oscar’s Culturally Competent Care Program- reducing healthcare disparities and improving access for the underserved population. Tamara holds a B.A. from the University of Cincinnati’s and M.B.A from Miami University.
Tamara Ward is the SVP of Insurance Business Operations at Oscar Health, where she leads the National Network Contracting Strategy and Market Expansion & Readiness. Prior to Oscar she served as VP of Managed Care & Network Operations at TriHealth in Southwest Ohio. With over 15 years of progressive health care experience, she has been instrumental driving collaborative payer provider strategies, improving insurance operations, and building high value networks through her various roles with UHC and other large provider health systems. Her breadth and depth of experience and interest-based approach has allowed her to have success solving some of the most complex issues our industry faces today. Tam is passionate about driving change for marginalized communities, developing Oscar’s Culturally Competent Care Program- reducing healthcare disparities and improving access for the underserved population. Tamara holds a B.A. from the University of Cincinnati’s and M.B.A from Miami University.


 Dr. Peter Walsh joined the Colorado Department of Health Care Policy and Financing as the Chief Medical Officer on December 1, 2020. Prior to joining HCPF, Dr. Walsh served as a Hospital Field Representative/Surveyor at the Joint Commission, headquartered in Oakbrook Terrace, Illinois.
Dr. Peter Walsh joined the Colorado Department of Health Care Policy and Financing as the Chief Medical Officer on December 1, 2020. Prior to joining HCPF, Dr. Walsh served as a Hospital Field Representative/Surveyor at the Joint Commission, headquartered in Oakbrook Terrace, Illinois.








